1 Federación Argentina de Cardiología. 2 Clínica de Especialidades Villa María, Córdoba, Argentina. 3 Hospital Italiano de Bu enos Aires, Argentina. 4 Insti- tuto Médico DAMIC / Fundación Rusculleda de Investigación en Medicina. Córdoba. 5 Instituto Médico de Alta Complejidad (IMAC), Salta, Argentina. 6 Establecimiento Asistencial Gobernador Centeno, General Pico, La Pampa. 7 Clínica Marañón, Villa María, Córdoba, Argentina. 8 Centro de Investigación y Tecnología de la Universidad Nacional de Villa María. Área de investigación, Escuela de Salud Pùblica, Universidad Nacional de Córdoba. 9 Hospital Dr. Cosme Argerich GCBA, Argentina. 10 Centro Médico Cardioterapia, Buenos Aires, Argentina. 11 Instituto de Cardiología "J. F. Cabral" Corrientes. Argen- tina. 12 Comité de Enfermedad Cardiovascular en la Mujer “Cesar M. Serra”, Federación Argentina de Cardiología.
Corresponding author’s address
Dra. Mildren Del Sueldo
Postal address: Calle Mendoza 1444, 5900 Villa María, Córdoba, Argentina
E-mail
Received on March 7, 2022 Accepted after review on April 5, 20222 www.revistafac.org.ar
There are no conflicts of interest to
disclose.
The Bayer Laboratory financed the survey through Mercoplus Latin America
Keywords:
Cardiovascular diseas.
Women’s health.
Risk factors.
Pregnancy complications.
Surveys and questionnaires.
ABSTRACT
Background: Cardiovascular disease (CVD) poses a major health problem for women in the world. Despite 30% of women dying from cardiovascular causes, in the country, data on the per- ception of this problem in the female population is scarce..
Objective: To identify the perception of women in Argentina on knowledge of CVD and pre- ventive behaviors, level of awareness of their own risk, and risk factors unique to women.
Method: In March 2020, a web survey was conducted on a sample of women from 5 Argen-tine cities.
Results: The results obtained from 1500 women surveyed showed that cancer was perceived as the main health problem, while violent death was identified as the leading cause of death. Only 11% identified cardiovascular disease as their main health problem and 16% as their leading cause of death. The proportion of women who have knowledge on cardiovascular risk factors was 96%, symptoms of the disease 75%, and preventive behaviors 98%. However, specially the younger ones underestimate this disease, feeling more threatened by violent death-homicide and cancer. The results also show that the main source of information was social networks and the internet, not medical advice..
Conclusions: In this sample of women in Argentina, they do not perceive cardiovascular disease as their main cause of disease and death. The work to increase their perception of the risk could result in a decrease in the morbidity and mortality that this disease entails, thus improving their quality and life expectancy.
INTRODUCTION
Cardiovascular disease (CVD), including coronary artery disease (CAD) and stroke, represents the main health problem for women in the Western world. The World Heart Federation reported that every year, 8.6 million women die all over the world due to CVD[1]. A recent report from the Lancet Women and Cardiovascular Disease Commission reports that 35% of all deaths in women at world level are due to CVD and that 275 million were diagnosed with this disease in 2019[2].
In Argentina, CVD is still the first cause of death. In year 2019, it was the cause of 31.3% of all deaths, which entails that one in every three Argentine women die by CVD[3]. In European countries, the problem is even greater, and 49% of women die due to CVD in comparison to 40% of men[4].
.
In spite of this evidence, there is in women from Western countries an erroneous identification about which is the main health problem for them, underestimating CVD as a threat and seeing it more as a health problem for men. In a survey form 1997, less than 30% considered that CVD was their main cause of death, and identified breast cancer as their most important health problem[5].
In Latin America, three surveys reported that the identification by women of CVD as main health problem or first cause of death was less than 20%, with sample units form capitals or nearby urban areas assuming a similar knowledge in the interior of each country[6,7,8].
These data have motivated the creation of programs addressed to change this perception by women, as “Go Red for Women” (American Heart Association) and “Mujeres en Rojo” (Federación Argentina de Cardiología – Argentine Federation of Cardiology) in Argentina. Specific programs about awareness and education have achieved for 54% of US women to identify CVD as their main enemy, although ethnical and racial differences have been observed[9].
Undoubtedly, making such differences is the first step to identify the obstacles that limit awareness and education not being delivered equally for all women. For this reason, the Committee on CVD in Women of the Federación Argentina de Cardiología (FAC) proposed performing this survey, with more national representation, extending it to the main capital cities in our country, which makes it a novelty. The proposed aims are the following ones:
1) to inquire into the degree of knowledge of women about CVD, symptoms, cardiovascular risk factors (CVRF) and behaviors that prevent or reduce the chances of getting sick;
2) to assess the perception and level of awareness that women have on their own risk of suffering and dying by CVD; and
3) to assess the CVRF that are unique to women such as menarche, menopause, pregnancy and related complications.
MATERIALS AND METHODS
Population
The unit of analysis was women with ages ranging from 20 to 70 years, living in Argentina (Buenos Aires’ suburban area/city of Buenos Aires, Córdoba, Santa Fe, Mendoza and Tucumán). The selection of the sample was randomized, following the population distribution in every city, and taking into account the age, and socioeconomic and education level of the represented population.
General study design – Instrument used
Observational, descriptive, cross-sectional study. The data collection instrument was a semi-structured questionnaire that had 11 blocks:.
Statistical analysis
The description of the measurable variables is presented as mean and standard deviation (SD) and categorical variables from percentage distribution.RESULTS
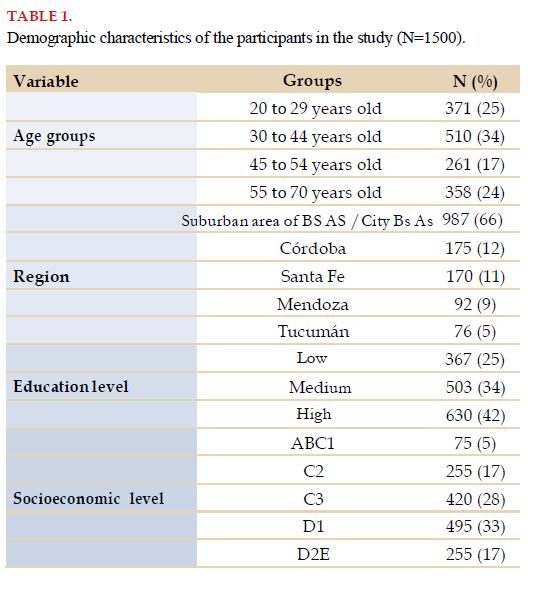
From the total of 1951 women surveyed, in this analysis 1500 were included with full data. The average age was 42±13 years; 81% stated having been pregnant, with an average of 3 (Q1=2 and Q3=4). About the number of children, a mean of 2 children was obtained (Q1=2 and Q3=3).
Sixty-six percent was living in the city of Buenos Aires or its suburban area, 57.6% had health coverage by medical insurance or prepaid medicine, 17% had a low SEL and 42% had a high EL (Table 1).
-Perception and knowledge of cardiovascular diseases in women.
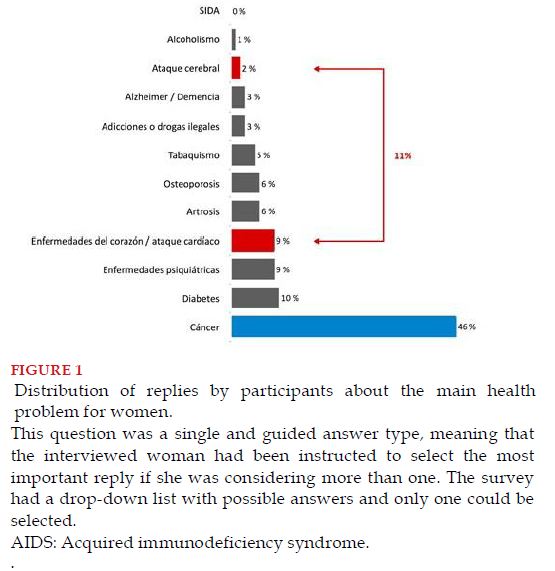
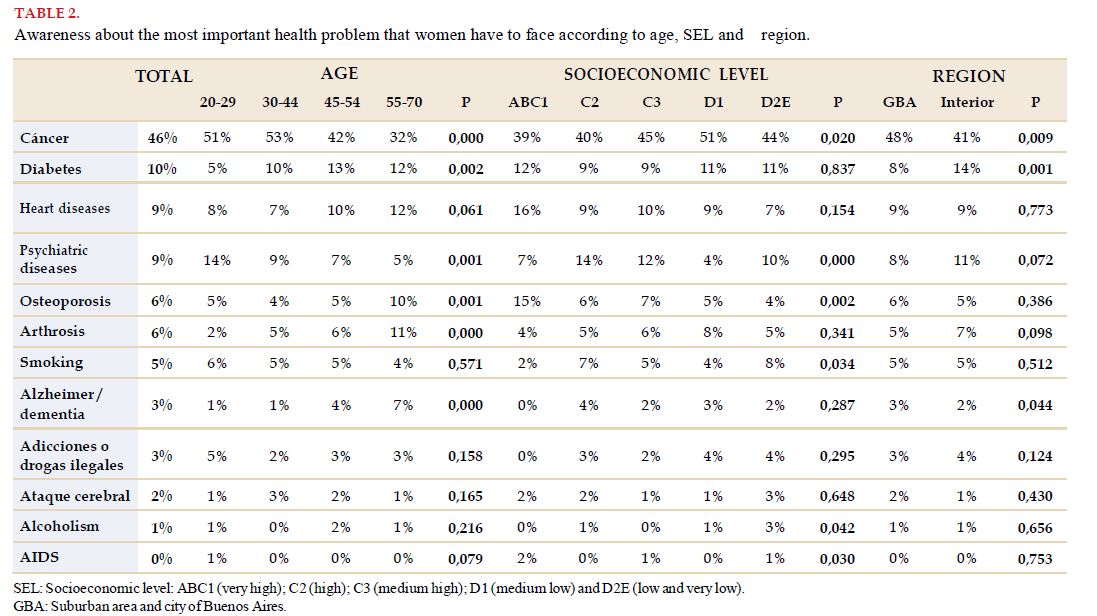
The surveyed women were asked to select between 12 diseases which they considered to be the main health problem women face (Figure 1). Cancer was indicated by almost half of them as the most important problem, while a minority (11%) proposed CVD as the main health problem (heart attack 9% and stroke 2%). In the analysis according to age, SEL and the region they inhabit, it was observed that the identification level of CVD as main health problem presented a trend (not significant) that increased as age increased and with a higher SEL (Table 2). Remarkably, more women with low SEL (44%), from the suburban area of Buenos Aires (48%) and younger ones (51%) perceived cancer as their main health problem significantly (p<0.05).
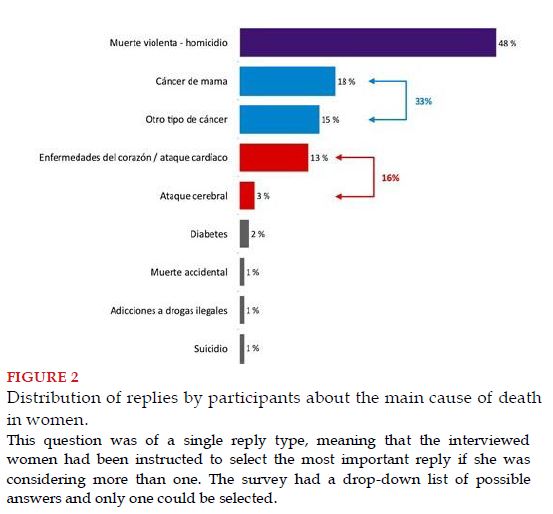
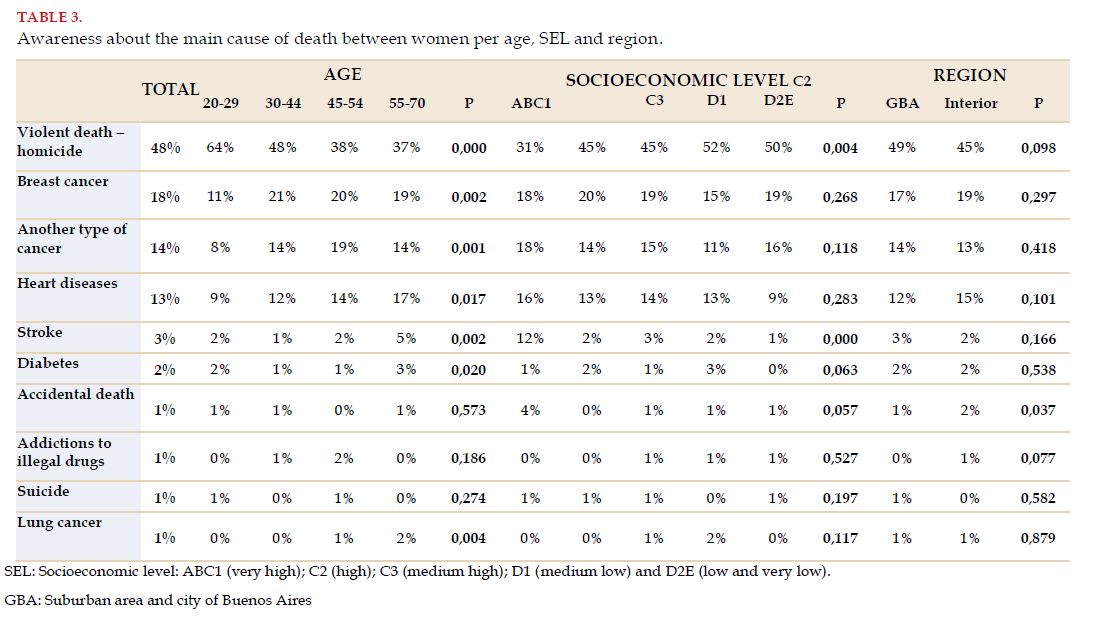
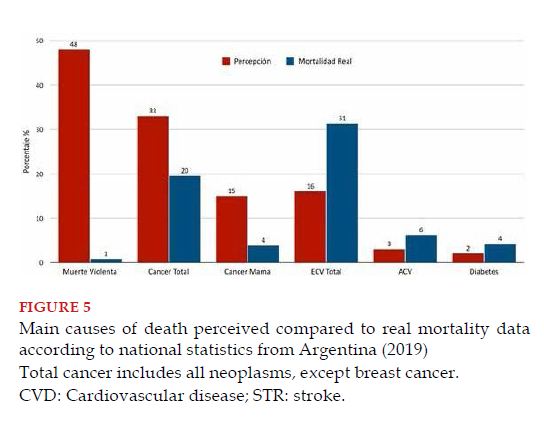
As a reply to the question: “What do you think is the main cause of death between women?”, surprisingly, 48% stated violent death/homicide, and cancer held a second place, while CVD was more relegated with 16% (Figure 2). Although a relationship was observed between more age (p<0.001) and higher SEL (p=0.002) with increase in the identification of CVD as the main responsible for death, the percentage was always less than violent death and cancer (Table 3).
-Self-perception of knowledge on CVD, CVRF and heart attack symptoms.
When faced with the question: “How would you describe your knowledge on CVD, in a scale from 1 to 5, where 1 means very scarce and 5 very substantial?”, more than half of women (52%) stated it was scarce or very scarce, 28% average, and 14% substantial or very substantial. The self-evaluation about the level of knowledge on CVD is superior between women older than 55 years (p<0.001), in those with greater SEL (p=0.02) and LE (p<0.001). There were no differences between the cities analyzed.
With regard to the knowledge of CVRF and their relationship with the development of CVD, it was verified that women in general know about their significance, since 96% assigned to them the same high scores of 4 and 5 points. Also, when asked about strategies to reduce CV risk, 98% of the women interviewed manifested that shedding weight, reducing cholesterol, quitting smoking, decreasing salt consumption and performing physical activity contributed significantly to prevention.
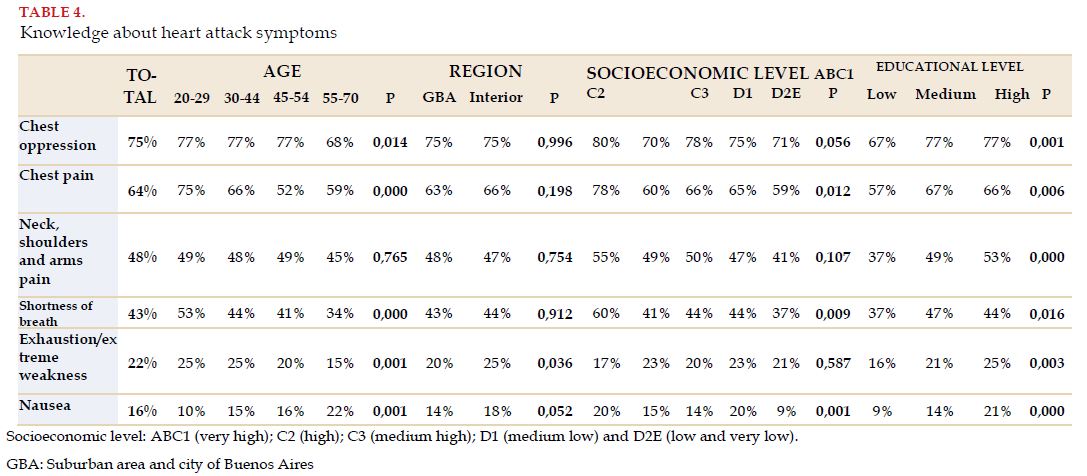
Faced with the questions, “What symptoms do you associate with having a heart attack?”, it became evident that women have knowledge on them, mainly typical symptoms as precordial oppression or pain. Less than half related pain in their arms, shoulders or neck and dyspnea with symptoms of heart attack, and only a minority identified the other symptoms that may appear in women in such a scenario. There were no differences in terms of age and the geographical region analyzed, but women with more SEL and EL identified more precordial oppression, pain in arms, neck or shoulders, shortness of breath and nausea as symptoms related to heart attack (p<0.05) (Table 4).
-Access to information about heart diseases.
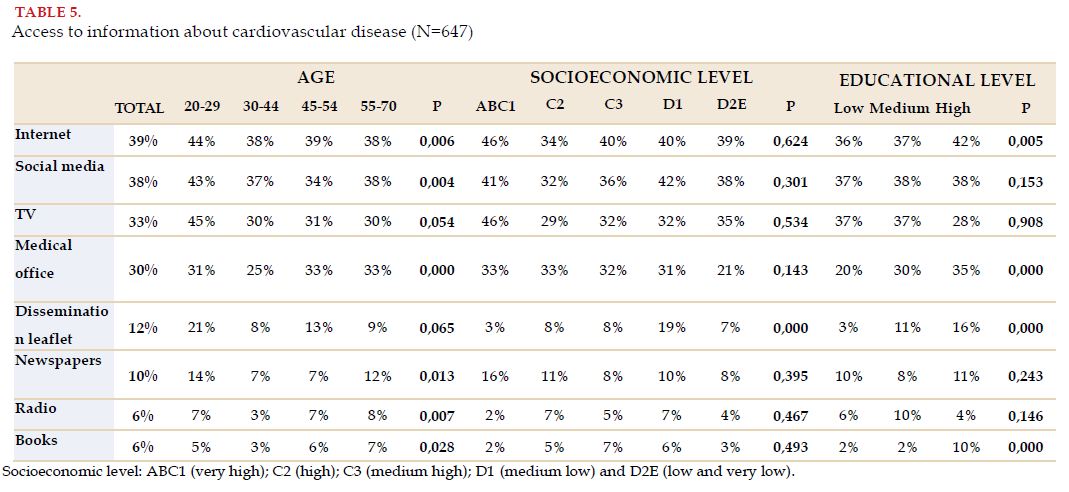
Faced with the question “Have you seen, heard or read information about heart diseases in this last year?” only 647 (45%) replied affirmatively. From this group, 39% did it through the Internet, and 38% by social media, while 30% received information from a health care professional. Access to information through the Internet and social media was more frequent in the group of younger women (p=0.006). More EL was associated to more access through the Internet (p=0.005), medical office (p<0.0001), dissemination leaflets (p<0.0001) and books (p<0.0001), while SEL did not show significant differences (Table 5).
-Time elapsed since the last medical appointment and specialty consulted.
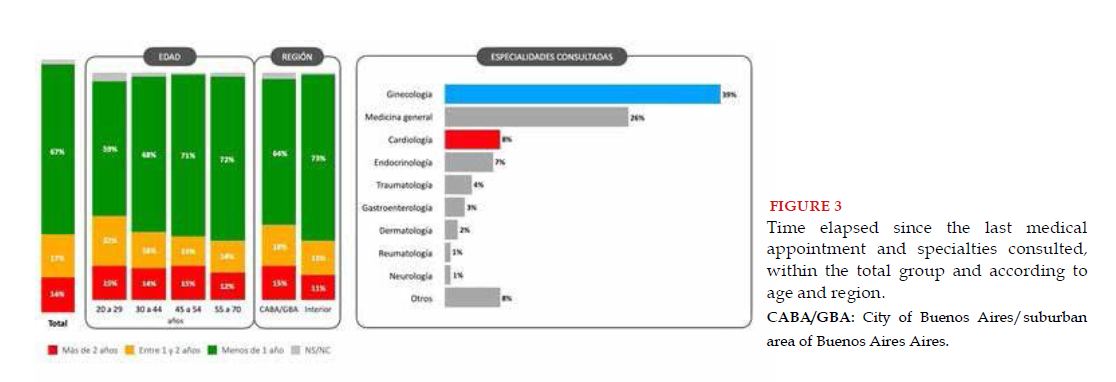
To the question, “When was the last time you visited a doctor?”, 67% replied within the last year, and in 65% the specialty consulted was gynecology or general medicine, while only 8% was cardiology (Figure 3). When asked about whether their physicians had informed them about CVD prevention measures or about cardiac symptoms, the answer was affirmative in 53% and 20%, respectively. But for women older than 55 years, who received more information from physicians (p<0.001), there were no significant differences observed between regions, EL and SEL. .
-Information related to menarche, menopause and pregnancy.
The average age of menarche was 12.4±0.78 years; 2.7% reported early menarche (<11 years). From the total of the sample, 33.7% were menopausal, at an average of 46.9±6.38 years. From these, 6% reported having stopped menstruating before 40 years and 20.2% before 45 years. The percentage of menopausal women was greater in women with early menarche (41.3 vs 32.9%; p=0.022), which occurred before 45 years of age in a similar percentage (25.4 vs 28.4%, p=NS).
To the question about whether women are more prone to suffering CVD after menopause, 67% replied that it was true, with no differences in terms of age, region or EL, but yes in relation to SEL (75% vs 58% between the highest and lowest SEL, respectively).
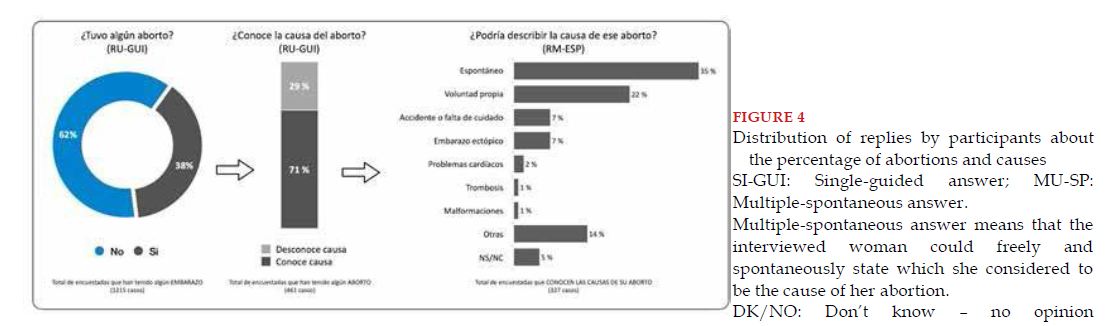
An important topic and rarely consulted about as part of CVRF in women are pregnancy complications. From the surveyed women, 81% stated having been pregnant with an average of 2.8 pregnancies; 59% increased their weight by more than 20% in comparison to before the pregnancy, with no difference by SEL, but with more prevalence between those with less EL, 72 vs 51% (p<0.0001); 24% had hypertension with no previous history, and equally, women with lower EL had more prevalence, 29 vs 21% (p=0.01); 9% were diagnosed with gestational diabetes, with no differences by SEL or EL; 18% had preterm deliveries before 37 weeks and 9% before week 34, with no significant difference per SEL or EL.
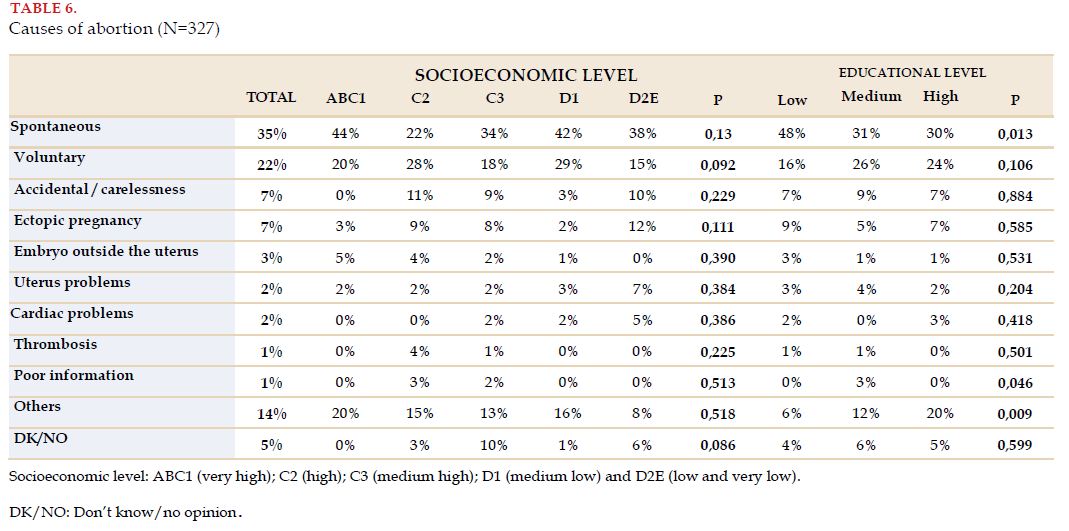
Thirty-eight percent reported having had an abortion, and 71% of them knew the cause of it, with no differences according to SEL or EL (Figure 4) (Table 6).
-Relationship between sociodemographic characteristics with identification of CVD as first cause of death.
Women ≥55 years identified CVD as the main cause of death with greater frequency than women younger than 55 years: 22.3 vs 12.1% (OR=2.07; 95% CI=1.57-2.74; p<0.001). A higher SEL (middle low, middle high, high and very high) showed a trend to association with more identification of CVD as the main cause of death than a lower SEL (low and very low): 37.4 vs 31.6% (OR=1.29; 95% CI=0.98-1.71; p<0.068). Women with more EL (complete secondary school or more) identified CVD as the main cause of death more frequently than those with a lower level: 15.7 vs 9.4% (OR=1.78; 95% CI=1.25-2.53; p<0.001).
The affirmative response to the question about having received information about cardiac diseases in women over the last 12 months was associated with more probabilities of identifying CVD as the main cause of death: 21.1 vs 9.1% (OR=2.66; 95% CI=2.05-3.46; p<0.001). However, between women that reported having obtained information, the percentage that identified CVD as the main cause of death was low, with no differences between those that received it from the Internet and social media, physicians or another source (21%; 26.5% and 18%; p=NS).
DISCUSSION
This analysis showed that current knowledge by Argentine women that CVD is the main cause of disease and death is highly deficient. This has not changed in spite of all efforts by two Argentine cardiology societies, which have been working from more than 15 years on this issue.
This reality presents a great challenge, not just for scientific organizations, but also for the sanitary authorities in our country, and requires the acknowledgement that only by joining forces and establishing it as a priority, awareness can be achieved in the female population.
In Argentina, according to the published statistics by the Ministry of Health of the Nation, corresponding to year 2019, CVD is the main cause of death in both genders, corresponding to 31.3% (48,530 deaths) in women and 29.7% (48,402 deaths) in men. The second cause in both genders is cancer, representing 20.4% (33,175 deaths) for men and 19.5% (30,252 deaths) in women, in whom the type that causes more deaths is breast cancer (3.8%; 5900 deaths). In other words, every 8 women that die by CVD, one will die due to breast cancer, and this ratio has remained so for several years[3,11].
On the other hand, it is known that from 2000 and 2010, cardiovascular (CV) mortality in Argentina was reduced by 22% (376 to 293 per 100,000 inhabitants), thanks to the implementation of interventions based on evidence, such as lifestyle modifications, advancements in diagnostic techniques, medications and CV interventions[12]. However, during the COVID-19 era in years 2020 and 2021, many of such advancements were dampened or even decreased. This is shown by a recent Argentine multicenter study, where it was possible to observe that the consultations caused by cardiovascular emergencies decreased 75% and hospital admissions 48%; admissions due to pain by coronary origin 62% and stroke 46%. This also happened with invasive procedures for the treatment of CAD[13,14].
Besides, as a consequence of less control of CVRF, from April to October 2020, up to 10,500 new cases of CVD may have occurred that could have been prevented[15]. Therefore, this reduction in CV mortality achieved in a decade, may not be so currently, and the figure reflecting mortality by CVD in women could be even bigger.
Undoubtedly, when analyzing these data, it would be expected for Argentine women to have more knowledge on this true threat and what CVD represents for them; but the results of this survey do not reveal so, manifesting a great discrepancy (Figure 5). Almost half of the surveyed women pointed out cancer as the most important health problem, and just a minority, one in ten, considered it to be CVD. Surprisingly, 48% prioritized violent death/homicide, followed by cancer (33%), relegating CVD to a third place. The level of knowledge of this reality was in both cases, directly proportional to age and SEL; that is to say, the greater the age and SEL, the more the knowledge, with the location of residence not being relevant.
LIMITATIONS AND STRENGTHS
This study presents limitations proper of this type of investigation. The survey was made through a Web platform, which may cause a selection bias in terms of accessibility to it, and the questionnaire used was based on previously used surveys on awareness, particularly by the AHA, which was created to be performed in another country with cultural, ethnic, financial and accessibility characteristics different from Argentina.
The main strength of this study is that it is the first made on awareness on CVD in women in a large sample size. The inclusion of women of the city of Buenos Aires and 5 provinces, without representation from another 18 provinces, rural areas and minorities may be considered a limitation for the extrapolation of data. This sample could be considered representative of urban areas in the most important capital cities of the country. However, considering the socioeconomic and cultural differences between the different regions of Argentina, it is likely for the results of this study to show a more optimistic view of national reality. Moreover, it included in the questionnaire, data about CVRF unique to women, about which there are very few data published in Argentina.
CONCLUSIONS
To conclude, awareness by Argentine women about CVD being their main cause of disease and death is still highly deficient, with a great discrepancy existing between perception and reality. br>
Although the degree of knowledge about the main CVRF, disease symptoms and preventive measures is high, it seems that this information is not related to the belief that they may get ill and die by this cause. These results show the need to continue and intensify campaigns of awareness about the impact CVD has on female health conducted by scientific societies, expanding them to intermediate and governmental organizations that may enable a larger scope. Having knowledge about the means through which information is acquired according to age, SEL and EL may help to be more effective with the message, to thus be able to reduce morbimortality by CVD in Argentine women.
ACKNOWLEDGEMENTS
The authors thank the Board of Directors (2020 and 2021) of the Federación Argentina de Cardiología for their unconditional support to perform this study, as well as all the members of the Committee of Cardiovascular Diseases on Women “Dr. Cesar Serra”.
Also, we thank the Bayer Pharmaceutic Company for making it possible to perform the survey.
BIBLIOGRAPHY