Images in Cardiology
Right atrial compression due to unilateral diaphragm paralysis and patent foramen ovale detected incidentally in sars-cov-2 pneumonia
Pablo M Corredoira1, Helena Rendón-Fernández2,
María Aguado-Aguado1,
BMaría C. Aured Guallar1.
1 Hospital Universitario Miguel Servet, Zaragoza (Spain). 2 Hospital Clínico Universitario Lozano Blesa, Zaragoza (Spain).
Corresponding author’s address
Dr. Pablo Manuel Fernández Corredoira
Postal address: López Allué Nº5 4º Dcha., 50005, Zaragoza, España.
E-mail
INFORMATION
Received on April 4, 2022
Accepted after review
on May 17, 2022 www.revistafac.org.ar
There are no conflicts of interest to
disclose.
Keywords:
SARS-CoV-2.
Patent foramen ovale
Long COVID.
Persistent COVID.
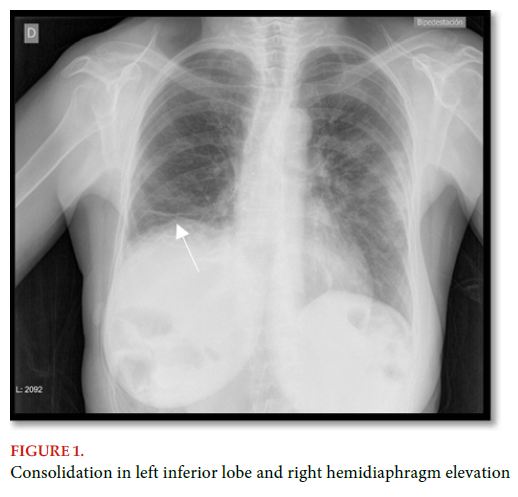
The case presented here is a 64-year-old woman. She was hypertensive and a smoker, who underwent thymectomy, presenting lesion in the right phrenic nerve. The patient went to the ER due to symptoms compatible with infection by SARS-CoV-2, finding SpO2 of 89-90% in a sitting position, which increased up to 96% in a supine decubitus position. Chest X-rays were taken, observing a peripheral consolidation in the left inferior lobe and right unilateral diaphragm paralysis (Figure 1). She was admitted for a brief period for the treatment of pneumonia due to SARS-CoV-2. Since after 5 months of convalescence she remained with dyspnea after moderate efforts, the test with spirometry was completed, finding a normal respiratory pattern and echocardiogram was requested to assess the RV, pulmonary circulation and E/e’ ratio, which were not pathological. In Figure 2, partial RA collapse is observed. The presence of patent foramen ovale (PFO) was confirmed by agitated saline echocardiography test with Valsalva maneuver, and subsequently by transesophageal echocardiography (Figure 3).


Right atrial collapse is a rare manifestation mainly caused by copious effusions of pleural or pericardial origin, and extracardiac tumors. There are few cases described in medical literature where right hemidiaphragm elevation is the underlying cause[1]. If there is concomitant PFO due to the increase in pressure on the RA, intracardiac platypnea-orthodeoxia syndrome develops, requiring percutaneous closure[2,3]. Nevertheless, both partial RA collapse and PFO are frequently casual findings in echocardiography with no manifest direct clinical symptoms, and therefore, in most cases, no treatment is necessary.
This case was interpreted as long COVID syndrome, with symptoms disappearing over the following months. Finally, no PFO closure was made.
BIBLIOGRAPHY
- Tayyareci Y, Bayazit P, Taştan CP, et al. Right atrial compression
due to idiopathic right diaphragm paralysis detected incidentally
by transthoracic echocardiography. Turk Kardiyol Dern
Ars 2008; 36: 412 - 414.
- Darchis JS, Ennezat PV, Charbonnel C, et al. Hemidiaphragmatic
paralysis: An underestimated etiology of right-to-left shunt
through patent foramen ovale? Eur J Echocardiogr 2007; 8: 259
– 2564.
- Lopez Gastón OD, Calnevaro O, Gallego C, et al. Sindrome platipnea-
ortodeoxia por foramen oval permeable, aneurisma del
septum interauricular y parálisis del hemidiafragma derecho.
Medicina (B Aires) 2005; 65: 252 - 254.