Instituto Médico de Alta Complejidad (IMAC), Salta, Argentina
Corresponding author’s address
Dr. Daniel A. Ormachea
Postal address: Adolfo Güemes 88, 4400 Salta Capital, Argentina.
E-mail
Received on March 29, 2022 Accepted after review on May 28, 2022 www.revistafac.org.ar
There are no conflicts of interest to disclose.
Keywords:
Thrombosis. Prosthetic valve
Thrombolytics. Surgery.
ABSTRACT
Prosthetic valve thrombosis is a rare but serious entity. The diagnosis of this entity must be made quickly, since it causes a torpid evolution, rapidly leading to heart failure and death. Currently, there is a debate between thrombolytic therapies versus surgical therapy as treatment, but due to the clinical presentation of the disease and the risks implied by each therapeutic management, it turns into a challenge for therapeutic choice.
INTRODUCTION
Prosthetic valve thrombosis is a rare but severe complication. It occurs when a thrombus adheres to a prosthetic heart valve or near it. It may obstruct blood flow or interfere with valve function, leading to a condition that is nearly always deadly. In terms of therapeutic condition, currently there is a dispute between thrombolytics and heart surgery; but due to the severity of this entity and the risks of every treatment, the decision will fall on the experience of the center and the clinical severity of the patient.
Next, we present a clinical case of mechanical prosthetic valve thrombosis.
CLINICAL CASE
Female, 64-year-old patient, from the city of Paraná (province of Entre Ríos), with history of permanent atrial fibrillation, ischemic stroke, hypothyroidism and mitral valve stenosis resolved by mechanical valve replacements, so she was anticoagulated with acenocoumarol.
She went to the ER due to FC IV dyspnea, with a one-month course, that had emphasized within the last 24 h.
In the physical examination, she presented BP 90/60 mmHg, muffled prosthetic sounds, tachypnea, crepitant rales and hypoventilation in both lung bases.
In the electrocardiographic recording, atrial fibrillation rhythm appeared, with moderate ventricular response; in chest X-ray there was increased cardiothoracic ratio, with signs of right overload and pulmonary blood flow redistribution.
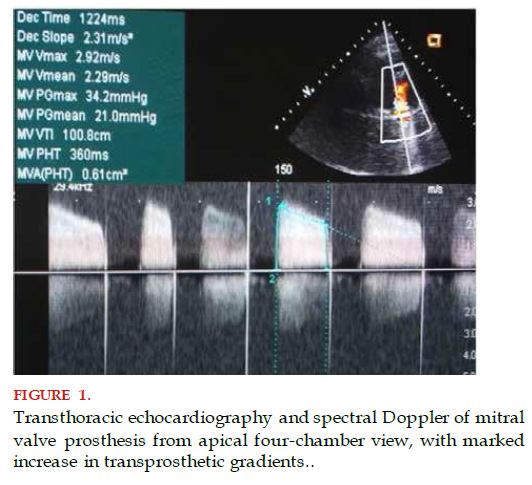
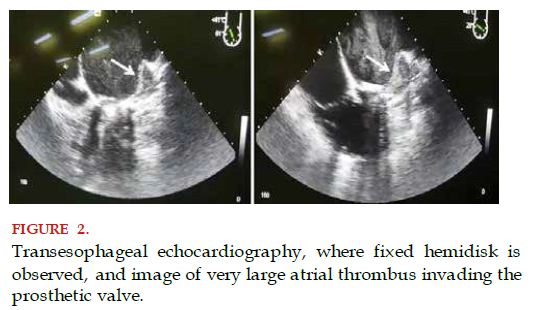
Transthoracic echocardiograms were conducted, which reported prosthetic mitral valve with elevated gradients. Absence of prosthetic posterior disk mobility was verified through transesophageal echocardiography; and thrombus image holding the left atrial lateral wall and appendage, and invading mitral valve posterior disk; peak gradient 34 mmHg, mean gradient 22 mmHg, mitral valve area by pressure half-time (PHT) 0.61 cm2, right chambers dilatation and severe pulmonary hypertension (70 mmHg pulmonary arterial systolic pressure - PASP) (Figures 1 and 2).
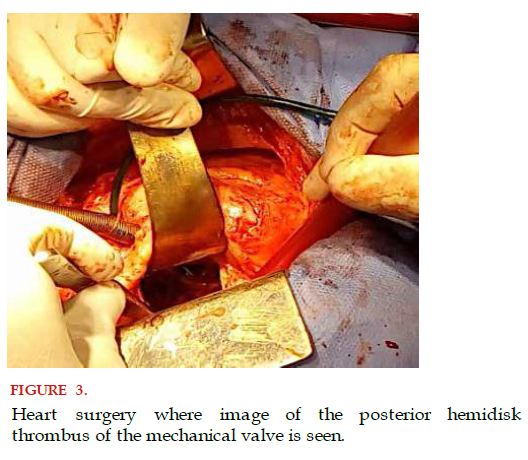
With the diagnosis of subacute thrombosis of the prosthetic valve and taking into account the large size of the thrombus, it was decided to adopt a surgical management, performing the extraction of the thrombus and no valve replacement. The thrombus was adhered to the left atrial wall that invaded the posterior hemidisk of the valve (Figure 3).
The patient coursed her postoperative period with no complications, with echocardiographic controls that showed decrease in trans-prosthetic gradients. She was discharged during the fifth day, before adjustment of anticoagulation with acenocoumarol.
DISCUSSION
The clinical case presented corresponds to a female patient who presented mitral valve prosthesis thrombosis, with a very large thrombus, which in spite of her hemodynamic state and her FC, required surgery that was successful.
Mitral valve prosthesis thrombosis is a rare complication (0.5-6%) and should be understood as a multifactorial phenomenon that covers surface, hemodynamic and hemostatic factors. Another point to take into account is the time of evolution of thrombosis[1].
The treatment, in terms of mortality, is of high risk, whichever the option chosen (surgical or thrombolytic). Currently, the treatment indications are of class IIa or IIb, but all with level of evidence C, which indicates that the measures taken are a medical challenge.
The recommendations proposed by the American Heart Association (AHA) guidelines are in regard to prosthetic valve thrombosis, indicating that fibrinolytic therapy should be preserved for patients in NYHA functional class III or IV and with high surgical risk[2].
However, the embolic and bleeding complications of thrombolytics and their therapeutic inefficacy are increased in the presence of a very large thrombus in the left chambers, to the extent that some important organizations advise emergency surgery in left prosthetic valves with very large thrombus (>0.8 cm2 or >1 cm2)[3].
A meta-analysis describes that therapy with fibrinolytics does not have a complete success rate, since besides reports having been made with small series of cases, recurrence rates and complications are 61.3% in patients in functional class IV; therefore, there should be no opposition to emergency surgery in patients in functional class IV[4].
BIBLIOGRAPHY