
Instituto de Cardiología del Sanatorio Británico SRL, Rosario, Santa Fe, Argentina.
Corresponding author’s address
Dr. Daniel A. Zanuttini
Postal address: Paraguay 40 – 2000, Rosario, Santa Fe, Argentina
E-mail
Received on March 16, 2022 Accepted after review on May 2, 2022 www.revistafac.org.ar
There are no conflicts of interest to disclose.
Keywords:
Coronary artery bifurcation.
Percutaneous transluminal angioplasty.
Drug-eluting stents.
Intravascular ultrasound.
ABSTRACT
Introduction: Transluminal Coronary Angioplasty (PTCA) with drug-eluting stents (DES) of coronary bifurcation lesions continues to be complex, with significant revascularization rates due to restenosis; however, it is a feasible option. The limitation of angiography on the anatomical and morphological elements of bifurcations, which have already shown prognostic value, is well known.
Objective: To assess the effectiveness of PTCA with DES optimized by intracoronary ul- trasound (IVUS) in coronary bifurcation and combined events of death, myocardial infarction (AMI), stroke or revascularization of treated lesions (RTL).
Methods: Retrospective, single-center, single-arm registry. From 11/2018 to 10/2021, 457 co- ronary angioplasties were performed, of which 84 consecutive patients with coronary bifurcation lesions underwent PTCA with IVUS-guided DES implantation.
Results: The patients were followed on average 324 ± 83 days. The mean age was 61.4 ± 18.3 years; male gender 82%, diabetes 27%; multivessel disease 88%; calcified lesion 13.6% in angiography and 27% by IVUS. Syntax Score <22 in 69.1%, 23-32 in 27.3%. The most frequent bifurcation was anterior descending-diagonal 53.5%. Implanted patients with provisional stent technique 78.5%. DES mean luminal area was 7.3 mm2 in the main vessel. Re-intervention with a balloon due to hypoexpansion and/or lack of wall apposition 22.6%. In-hospital evolution: 2 pts with sub-clinical infarction (2.4%). Follow-up: 1 pt with AMI secondary to stent thrombosis (1.2%) in revascularized lateral vessel. In-hospital and long-term mortality and stroke 0%. Two stents (1.9%) presented late thrombosis, implanted in the lateral vessel, without clinical event.
Conclusions: PTCA with DES optimized by IVUS guidance in coronary bifurcation lesions is a safe procedure, with a low incidence of major in-hospital and late complications. An optimal implantation of the stent has impact on the results of the procedure
INTRODUCTION
Approximately 15 to 20% of patients with coronary atherosclerotic stenosis present coronary bifurcation lesion[1]. Transluminal coronary angioplasty (TCA), introduced in 1977, and its technological advancements, made it possible to treat coronary artery lesions increasingly complex[2]. The percutaneous treatment of lesions in coronary bifurcation relates to complex procedures, and often, with suboptimal results due to immediate complications (occlusion, dissection, significant residual stenosis, flow alteration) in the lateral vessel, and restenosis in its evolution, generally significant, according to physiological evaluation[3,4,5], manifesting clinically as peri-procedure myocardial infarction and requirement of new revascularization. Different studies showed that the percutaneous treatment is feasible. Within the first years, with the use of balloon catheter the results were discouraging. With the conventional stents, an improvement is observed, with significant decrease of major cardiac events. The development of drug-eluting stents (DES) allowed to obtain more favorable results, with more efficacy in restenosis prevention. Stenosis in the bifurcation areas of coronary arteries adds more complexity to procedures, with more chances of presenting complications, decrease in primary success rates and greater frequency of events in the distant follow-up. This type of lesions is classified according to the involvement of the related anatomical segments; however, the different classifications used ignore a series of fundamental anatomical and morphological elements, that have already proven their prognostic value. For this reason, auxiliary methods with intracoronary images, such as intravascular ultrasound (IVUS) and optical coherence tomography (OCT), become important to define the complexity of the lesion, and therefore, guide the technical choices during the procedure.
The aim of this study is to evaluate the effectiveness, safety and distant evolution of TCA with DES optimized by IVUS in patients with severe atherosclerotic disease in coronary bifurcation.
MATERIALS AND METHODS
Design of the study and selection of patients
This study is a retrospective, single-center and single-arm registry. Between September 2018 and October 2021, in the Department of Interventional Cardiology of the Cardiology Institute of the Sanatorio Británico SRL of the city of Rosario, a total of 457 coronary angioplasties were performed. From the total, 84 consecutive patients were identified with coronary bifurcation lesion, who underwent TCA with DES implant guided by IVUS.
Definition of bifurcation, classification and endpoints
The procedures were carried out according to the current guidelines[6]. The coronary bifurcation lesion is classically defined by the presence of stenosis ≥50% within the 3 mm of the carina (or center) of the bifurcation, and it may affect one or more anatomical segments, included the proximal main branch, the distal main branch and the side branch[5]. Bifurcation lesions are classified according to the involvement of the related anatomical segments. With this aim, the Medina classification was applied, which grants each segment (proximal main branch, distal main branch and side branch) a binary value of 1 or 0, representing respectively, the presence or absence of significant obstruction. The “true” bifurcation lesions are defined by compromise (stenosis ≥50%) of the two bifurcation branches (main and side branches), and are identified by the types of the Medina classification: 1.1.1, 1.0.1 and 0.1.1[5,7,8].Intravascular ultrasound (IVUS)
For the acquisition of IVUS images, a monoelement rotational displacement transducer was used with a frequency of 40 MHz, within a sheath a 2.6 F profile, with motorized pullback in an automatic traction system at 0.5 mm/seconds, connected to a commercially available scanner (Volcano Therapeutics Inc.)[19]. The stent lumen area and the branch (external elastic membrane) of the analyzed segment were determined millimeter per millimeter by computerized planimetry. In the qualitative analysis, the incomplete stent apposition was defined as the separation of at least one of its struts from the vascular wall, not involving a bifurcation area and the identification of blood flow behind the struts[20,21].Statistical analysis
In the descriptive statistical analysis, categorical variables are expressed as absolute and percentage frequencies. The continuous variables are expressed as mean±standard deviation. Angiographic and ultrasound comparisons were made, testing the differences in parameters of the continuous variables location, by student’s t-test. For this analysis, the SPSS 13.0 for Windows and EpiCal 2000 were used.
RESULTS
In the period from September 2018 to October 2021, 84 consecutive patients, with coronary bifurcation lesion, were treated with TCA with DES guided by IVUS in the main branch. The clinical characteristics are described in Table 1. The average age was 61.4±18.3 years, 82% of patients were males. Diabetes mellitus was present in 27.3%, hypertension in 45%, dyslipidemia in 52.3%. The most frequent clinical diagnoses in admission were acute coronary syndrome (ACS) in 34.5% and chronic coronary syndrome (CCS) in 26.1%. Vascular access was performed through the radial artery in 82.2% (69 TCA), with a 6 Fr or 7 Fr introducer, and 17.8% (15 TCA) by femoral artery access with a 7 Fr introducer.
Quantitative coronary angiography.
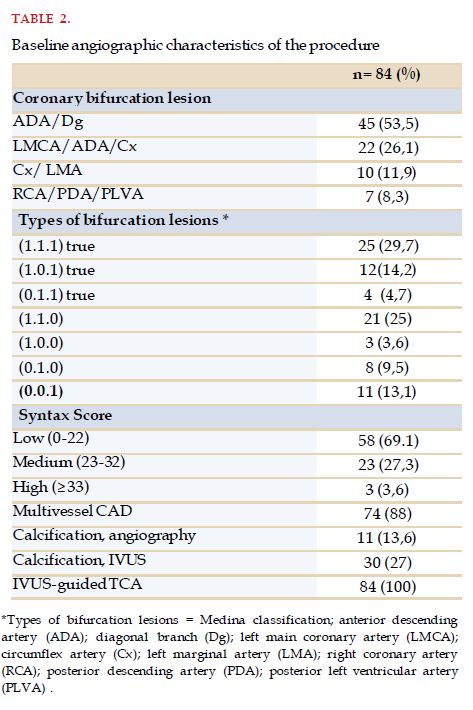
Table 2 shows the angiographic characteristics. The most frequent treatment for bifurcation lesion was the anterior descending artery and diagonal artery in 53.5% (45 lesions), left main coronary artery bifurcation in 26.1% (22 lesions), circumflex and marginal arteries in 11.9% (10 lesions) and distal right coronary artery, with posterior descending branches and/or posterior ventricular branches in 8.3% (7 lesions). The true coronary bifurcation lesions by angiography were 48.8% (41 bifurcations), and after IVUS evaluation, 8 bifurcation lesions were detected, presenting severe lesion considering the minimal lumen area in the main branch and/or side branch, modifying the initial treatment strategy. In 88% of cases (74 pts) there was multivessel CAD. In regard to angiographic complexity, 69.1% were low Syntax Score and 27.3% intermediate score. Calcification in coronary bifurcation lesion was identified in 13.6% (11 pts) in angiographic evaluation, increasing to 27% (30 pts) in IVUS evaluation
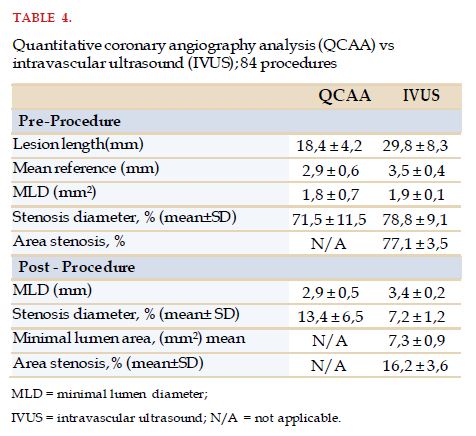
Table 3 shows the technique used in the procedure and its immediate results. Pre-dilatation with balloon was conducted in 82.1% (69 pts) of lesions, in 34.5% (29 pts) high-pressure noncompliant (NC) balloons were used to improve the preparation of the lesion based on the information by the IVUS. The pre-stent Kissing Balloon technique was performed in 14.2% (12 pts). The choice of the balloon diameter was in relation to the distal reference diameter visualized by IVUS. The mean reference diameter of the main branch was 2.9±0.6 mm and 3.5±0.4 mm, and the mean length of the main branch lesion of 18.4±4.2 and 29.8±8.3 mm, in angiographic evaluation and by IVUS, respectively. The mean angiographic diameter of the side branch was 2.4 mm. IVUS was performed in side branch in 7 bifurcation lesions.
Post-dilatation and use of the POT (Proximal Optimization Technique) technique was performed in all patients, regardless of angiographic information; and the final Kissing balloon technique in 100% of the bifurcation lesions treated with two stents and in 77.3% (65 pts) of those treated with provisional stent.
The most used strategy was the provisional stent in 78.5% (66 TCAs). The implanted DES were 102: 66 with the provisional stent technique, 19 Ultimaster®, 18 Firehawk®, 10 Orsiro®, 9 Resolute®, 6 Xience®, 4 Promus®. The 36 implanted DES with the two stents technique were 16 Ultimaster®, 12 Firehawk®, 4 Orsiro®, 4 Resolute®. The strategies applied were mini-crush, T-stenting, Culotte and DKC (Double Kissing Crush). The mean diameter and implanted stents length in the main branch were 3.01±0.5 mm and 32.12±6.2 mm, respectively. The mean diameter and implanted stents length in the side branch were 2.31±0.6 mm and 18.12±3.2 mm, respectively. Angiographic success in the main branch was obtained in all patients, and when correlating with IVUS, the initial success was 77.4% (65 pts), and in the other patients (22.6%), a reintervention was necessary with balloon, with more diameter or with more pressure, to reach the success criteria by IVUS in terms of good expansion and strut apposition in the arterial wall. The final mean lumen area of DES in the main branch was 7.3 mm2. Angiographic success in the side branch was obtained in 96.4%; the complications were 1 occluded side branch and 2 patients with dissection and TIMI flow <3.
Table 4 presents the results of the serial analysis of patients comparing quantitative coronary angiography with IVUS in the main branch.

Hospital clinical results
During in-hospital evolution, two patients presented significant increase in post-procedure troponins, confirming the diagnosis of sub-clinical myocardial infarction (2.4%). In 1 pt, LRV was possible, and the second pt continued with occluded side branch. No patient evolved with death, stroke or urgent myocardial revascularization surgery.
Clinical follow-up in all patients
The post-procedure clinical follow-up data were obtained in all patients. In an average period of follow-up of 324±83 days, 1 pt presented AMI secondary to subacute stent thrombosis (1.2%) implanted in side branch, and required revascularization of the treated lesion (1.2%). No pt evolved with death or stroke or myocardial revascularization surgery in this period. One pt presented side branch occlusion, treated with provisional stent, with no clinical event (Table 5).

DISCUSSION
This study, carried out in a center of Argentina, shows that angioplasty with DES implant in coronary bifurcation lesions guided by IVUS is a feasible, safe procedure, that optimizes the immediate and distant final result, since although the angiographic success observed in the main branch was 100%, and in the side branch 96.4%, after making the review with IVUS in the main branch, a reintervention had to be conducted in 22.6% of cases with a balloon with more diameter or pressure to reach the success criteria by IVUS in terms of good expansion and apposition of struts to the arterial wall. The pre-procedure evaluation also allowed us to better know the atherosclerotic plaque and bifurcation lesion morphology, markedly helping the process of choosing a treatment strategy, oriented to the use of non-compliant balloons in pre-dilatation and/or post-dilatation.
In regard to the classifications previously used, Medina’s ignores some characteristics such as lesion extension, branch size, corresponding myocardial territory, distribution and plaque load, angulation between branches (Y-type bifurcations: distal angle <70 degrees or distal T-type angle >70 degrees), tortuosity, calcification and thrombus. For this reason, auxiliary intracoronary imaging methods such as IVUS and OCT become significant. In the present series of cases, the presence of true bifurcation in angiographic evaluation was just 48.8% (41 bifurcations), and after evaluation with IVUS, 8 bifurcations were detected with severe lesion, considering the minimal lumen area in the main branch and/or side branch, suggesting a greater number of true bifurcations by this method, and modifying the initial strategy of treatment. Calcification was 13.6% (11 pts) in angiographic evaluation, increasing to 27% (30 pts) by IVUS.
The strategies for coronary bifurcation lesion revascularization are controversial. Previous dilatation of the side branch as the initial step of the procedure (regardless of the technique used) is still being discussed, since it may cause compromise and subsequent access problems when implanting the stent in the main branch in the case of the provisional strategy[22,23]. One of the recommended techniques for post-dilatation of the segment proximal to the carina, with the aim of optimizing expansion and stent apposition in this segment, is that known by the acronym POT (Proximal Optimization Technique), which includes the performance of an individual post-dilatation with a short NC balloon, with a size according to the diameter of the main branch proximal to the carina, before crossing the guidewire again toward the side branch, since balloon expansion would provide more opening of the stent struts in this location, facilitating recrossing[24,25]. This procedure can also be applied in two-stent strategy. The final post-dilatation with two simultaneous balloons (kissing) has been considered a critical procedure for the success of TCAs in bifurcations with 2-stent techniques, with lower rates of restenosis of the side branch and LRV[18,26,27]. On the contrary, the systematic performance of kissing-balloon after treatment with a single stent is still controversial. It is justified because this procedure adapts the stent of the main branch to the side branch orifice, correcting possible stent distortions, and optimizing stent expansion and apposition to the carina[23,28].
In a meta-analysis, the clinical results of different TCA techniques in coronary bifurcation lesions were compared. There were 21 controlled, randomized trials that included 5711 patients treated with 5 TCA techniques for bifurcation lesions: placement of provisional stents, placement of two-stents in T/T and protrusion, crush, culotte and DKC. In a 12-month follow-up, patients treated with the DKC technique presented less MACE (Major Adverse Cardiovascular Event) occurrence (OR 0.39; CI 95%, 0.26 to 0.55) in comparison to those treated with provisional stent, due to reduction in LRV (OR 0.36; CI 95%, 0.22 to 0.57); while no significant differences were observed in cardiac death, AMI and stent thrombosis. A clinical benefit was observed from the 2-stent techniques over the placements of provisional stents in bifurcation lesions in the side branch, with a ≥10 mm length[29].
The DEFINITION II trial also performed a randomized and multicenter comparison of two-stent and provisional stent techniques in 653 patients with complex coronary bifurcation lesions in 49 international centers. In a 1-year follow-up, TLF (target lesion failure) occurred in 37 patients (11.4%) and 20 (6.1%) in the provisional and two-stent arms, respectively (HR 0.52; CI 95%, 0.30-0.90; P = 0.019), driven to a large extent by the increase in AMI frequency (7.1%; HR 0.43; CI 95%, 0.20-0.90; P = 0.025), and TLR (target lesion revascularization) defined by clinical criteria (5.5%; HR 0.43; CI 95%, 0.19-1.00; P = 0.049) in the provisional group. A year after the indexed procedures, the incidence of cardiac death was 2.5% in the provisional group and 2.1% in the two-stent group (HR 0.86; CI 95%, 0.31-2.37; P = NS). The authors concluded that the systematic approach with two stents was associated to significant improvement in the clinical results in comparison to the provisional stent approach[30].
The ADAPT-DES registry was designed to determine the frequency, time and correlations of stent thrombosis and adverse clinical events after DES. A multivariate analysis was conducted, adjusted by propensity to examine the relationship between IVUS orientation and results at 1 year. In 3349 patients (39%), complex TCA was guided by IVUS, and devices with larger diameter, longer stents and/or higher inflation pressures were used in 74% of cases. The orientation of IVUS in comparison to orientation by angiography was associated to smaller rates of definite/probable stent thrombosis within 1 year (0.6% vs 1.0%; P = 0.003), myocardial infarction (2.5% vs 3.7%; P = 0.004) and composite MACE (3.1% vs 4.7R, P = 0.002)[25,31]. The benefits of IVUS were particularly evident in patients with acute coronary syndromes and complex lesions, although there were significant reductions in MACE in all the subgroups of patients, including stable angina and single-vessel disease, or stent thrombosis (3.1% vs 4.7%, P = 0.002). ADAPT-DES is the largest study on IVUS, according to previously developed data, and thus IVUS was associated to a reduction in stent thrombosis, myocardial infarction and MACE within 1 year after TCA with DES guided by IVUS. Subsequently, the investigators made a multivariate analysis, adjusted by propensity to examine the impact of IVUS guidance on results within 2 years, reporting that TCA guided by IVUS in comparison to TCA guided only angiographically was associated to reduced rates in 2 years of MACE (4.9% vs 7.5%; P = 0.003), definite/probable stent thrombosis (0.55% vs 1.16%; P = 0.003) and AMI (3.5% vs 5.6%; P = 0.0006).
According to a historical analysis, IVUS-guided angioplasty in comparison to angiographic-guided angioplasty was also associated to significantly smaller rates of MACE, AMI, stent thrombosis and LRV between 1 and 2 years after implant of DES. The average number necessary to treat with IVUS to prevent a MACE was reduced from 64 per year to 41 in 2 years[32].
In the ADAPT-DES, early improvement in survival free of events after IVUS-guided DES implant in comparison to angiography increased even more in a longer follow-up, of 2 years[26,31].
LIMITATIONS
This is a single-arm, single-center, observational and non-randomized study. The information reported is confirmatory of the results obtained in controlled clinical trials on the benefits of IVUS-guided stent implants in coronary bifurcation lesions. However, it allows to establish, in a complex scenario for interventionist cardiologists, that results similar to those reported in international excellence centers can be obtained in Argentina. Nevertheless, the size of the sample could be insufficient to evaluate the safety results.
CONCLUSIONS
In this analysis, involving patients of daily practice, with atherosclerotic coronary bifurcation lesions, drug-eluting stents implant guided by IVUS proved to be effective and safe, improving the end result of the procedure in nearly one in every four patients, with a rate of death and MACE in clinical follow-up significantly inferior to that reported in large controlled clinical trials with patients with similar complexity. No acute stent thrombosis was observed, and only 1 case of late thrombosis, similar to what has been described in recent papers. For all of this, it is recommended, based on sound evidence, for DES implants in coronary bifurcation lesions to be systematically guided by IVUS.
BIBLIOGRAPHY