1 Servicio de Cardiología, Hospital General Universitario de Valencia, Valencia, España. 2 Servicio de Urgencias, Hospital General Universitario de Valencia, Valencia, España.
Corresponding author’s address
Dr. Julián Abdala Lizarraga
Hospital General Universitario de Valencia.
Postal address: Avenida tres creas 2. 46014. Valencia. España.
E-mail
Received on March 17, 2022 Accepted after review on May 28, 2022 www.revistafac.org.ar
There are no conflicts of interest to disclose.
Keywords:
Acute coronary syndrome.
Spontaneous coronary artery dissection.
Coronary artery disease.
ABSTRACT
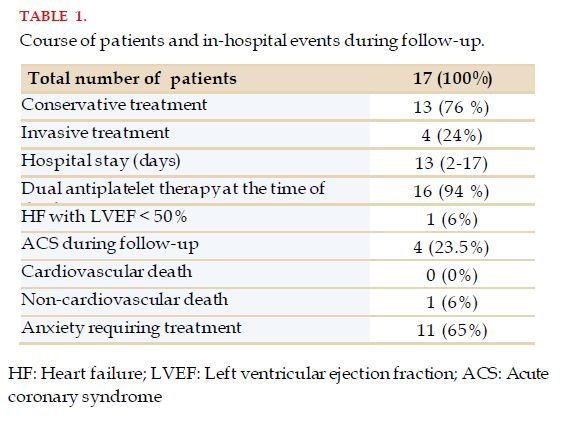
Spontaneous coronary artery dissection (SCAD) is a rare cause of acute coronary syndrome (ACS). The objective of this brief communication is to describe a 5-year experience in one center on SCAD patients. We conducted a prospective observational study on patients diagnosed with SCAD from 2016 to 2021 in our hospital. A total of 17 patients were included, of whom 82.4% were women with a mean age of 51+/-10 years old. Among the most prevalent cardiovascular risk factors were smoking and high blood pressure. Only 29.4% of the patients had a predisposing risk factor and 17.6% a precipitating factor. The most frequent clinical presentation was ST-elevation myocardial infarction (70.5%). In most of the coronary angiographies performed, a single artery was affected, being the left anterior descending artery the one most frequently involved. The majority of patients received conservative treatment. Treatment at discharge consisted of dual antiplatelet therapy (94.1%), beta-blockers and statins (88.2% in both cases) and angiotensin-converting enzyme inhibitors (47.1%). After a follow-up of one year, only one patient developed heart failure; and 23.5% of patients suffered a new ACS. Only one patient died from non-cardiovascular causes. SCAD is a serious disease that has a reasonable late prognosis in most cases.
INTRODUCTION
Spontaneous coronary artery dissection (SCAD) is a rare cause of acute coronary syndrome (ACS). There is no consensus about its pathophysiology or therapeutic management.
The aim of this brief communication is to describe the 5-year experience in a single center, on patients with SCAD.
METHODS
A descriptive, prospective, observational study was conducted on the epidemiological, clinical, diagnostic, therapeutic and prognostic characteristics of patients with diagnosis between January 2016 and January 2021, at the Hospital General Universitario de Valencia, Valencia, Spain.
RESULTS
A total of 17 patients were included, of whom 82.4% were women, with an average age of 51±10 years old. Between the most prevalent cardiovascular risk factors within the sample, there was smoking and hypertension, affecting 47.1% and 35.3% of patients, respectively. Only 29.4% of them had some predisposing factor, with puerperium standing out as the main one, and only 17.6% had some precipitating factor, with moderate intense effort being the most frequent one.
DISCUSSION
SCAD refers to a non-traumatic or atherogenic tear of the coronary arterial wall. It is responsible for 0.1% to 4% of SCAD cases[1].
It mainly affects young and postmenopausal women, with an average age of 51.8 years[2]. SCAD may also occur in men, presenting earlier than in women[2].
The underlying mechanism of this pathology is not entirely defined, but cases have been described, secondary to intimal tears of the arterial wall or spontaneous bleeding in the coronary vasa vasorum.
In most cases, it is possible to identify a predisposing systemic arterial disease; however, up to 20% of cases are idiopathic. Within the predisposing factors, we should consider fibromuscular dysplasia, postpartum period, multiparity, connective tissue diseases, systemic inflammatory diseases and hormone therapy[3].
In up to half of SCAD cases, it is possible to identify a precipitating factor, among which we find intense exercise, emotional stress, giving birth, activities inducing Valsalva maneuver, recreational drugs and hormone therapy[1,3].
The clinical presentation of this pathology is similar to atherothrombotic ACS, with chest pain being the most usual presentation. Patients with SCAD usually start with acute myocardial infarction (AMI). From them, 25-50% present ST-elevation myocardial infarction, and the rest with no-ST elevation, and a minority with unstable angina. In some cases, SCAD may present as cardiogenic shock, ventricular arrhythmias or sudden cardiac death[1,4].
The most relevant test to diagnose this disease is coronary angiography. Reviews on angiographic data obtained from these patients suggest that the most commonly affected artery is the anterior descending artery, which are usually affected in the middle-distal segments; and most patients usually present a single affected vessel. However, the compromise of non-contiguous coronary segments is not rare[1]. Among the diagnostic angiographic criteria, the presence of non-iatrogenic dissection, in absence of coronary atherosclerosis, is included.
In the patients in whom the diagnosis cannot be confirmed by coronary angiography or when percutaneous revascularization is to be performed, it is possible to use intracoronary imaging techniques, such as intravascular ultrasound or optical coherence tomography to visualize the dissection. Cardiac magnetic resonance or computerized axial tomography in coronary arteries should not be used as first-line diagnostic techniques, since they present many false negatives[5].
The aim of the treatment of patients that present SCAD is restoring coronary circulation and preserving myocardial function. The success of percutaneous coronary intervention (PCI) in such scenario ranges between 50 and 70%, and long-term complications may affect up to 70% of patients intervened. PCI in these patients is usually more complex due to vessel fragility, the difficulty of making the guidewire advance through true lumen, and the need to use very long stents to completely cover the lesions[1,5].
Due to most patients suffering SCAD recovering within 30 days with no treatment, the current trend is to prioritize a conservative treatment whenever possible[1,5,6]. In the cases where there is hemodynamic instability, ventricular arrhythmias, coronary occlusions or refractory ischemia, percutaneous or surgical revascularization could be considered.
Revascularization surgery is usually saved for cases where PCI has failed or is not technically feasible. In-hospital prognosis of these patients is usually similar to the patients managed with a conservative treatment, and better than those managed with PCI[1,5].
About pharmacological treatment, this should be addressed to relief residual symptoms in the affected patients, to prevent complications and recurrence of the disease. Although there are no randomized studies about it, patients with left ventricular dysfunction should be treated according to clinical practice guidelines for heart failure. Particularly, beta blockers have been associated to SCAD recurrence decrease in a multivariate analysis[1]. Lipid-lowering therapy should be kept for patients that require it due to hyperlipidemia or as preventive treatment. Anticoagulation or glycoprotein IIb-IIIa inhibitors should be suspended, unless there is intraluminal thrombus or some other indication for their use. About antiplatelet therapy, patients in whom PCI is conducted, should receive dual therapy according to clinical practice guidelines. However, there is a controversy surrounding antiplatelet therapy in patients managed with conservative treatment. Some authors propose using dual antiplatelet therapy for one year; while others recommend a strategy of short-term dual therapy, or just simple antiplatelet therapy for one year, with no sound evidence favoring either of them[1].
As to the prognosis of the disease, the in-hospital mortality reported is 4.2%, and the rate of in-hospital events is 8.8%, with recurrent AMI and revascularization requirement being the most frequent ones[1,5,6].
To conclude, SCAD is a severe pathology that may present a reasonably late outcome in most cases.
BIBLIOGRAPHY