Fundación Médica de Río Negro y Neuquén, Argentina.
Corresponding author’s address
Dr. Alberto Canestri
Postal address: Gobernador Anaya 4028, 8300 Neuquén, Argentina
E-mail
Received on March 9, 2022 Accepted after review on May 18, 2022 www.revistafac.org.ar
There are no conflicts of interest to disclose.
Keywords:
Retrospective study.
On/off pump.
Bilateral internal mammary artery graft
ABSTRACT
Objectives: To describe our off-pump coronary artery revascularization and results.
Material and methods: Retrospective study with 90 patients, with off-pump coronary artery surgery, performed by a single cardiac surgeon between September 2017 and August 2020, who changed his routine from on-pump and venous grafts to off-pump and bilateral internal mammary artery grafts.
Results: Mortality was 2.2% at 30 days. Patients were mostly male, with unstable angina and an average age of 63 years old.
Conclusions: Off-pump coronary artery bypass surgery is a safe procedure that can be performed in almost every patient with acceptable results, even if the previous surgeon’s technique was on pump.
INTRODUCTION
There are numerous studies comparing on and off-pump coronary artery surgeries, and using exclusively venous or arterial grafts. Most conclude that off-pump surgery and bilateral internal mammary artery grafts are more demanding for the surgical team and more beneficial for patients; while with on-pump coronary artery surgery more bypasses are done per patient, with less complications in anastomosis. This communication shows personal experience on 90 CAD patients intervened over a three-year period, of a surgeon that changed routine on-pump surgery to 100% off-pump surgery and bilateral internal mammary artery grafts procedures.
The aim of this study is to share the technique used and show the results in the short term of the surgical procedures.
MATERIALS AND METHODS
In the cardiovascular surgery service of the Fundación Médica de Río Negro y Neuquén, an average of 300 central interventions are made per year. Approximately, 65% are myocardial revascularization surgeries (MRS).
Over a term of 3 years, from September 2017 to August 2020, 90 pure off-pump coronary artery surgeries were conducted. They comprise the volume of surgeries by a surgeon that changed routine on-pump MRS and customary use of venous grafts to off-pump surgeries and mainly arterial revascularization.
Surgical technique.
After performing median sternotomy, the dissection of one or both skeletonized internal mammary arteries (IMA) and the internal saphenous vein is conducted, if necessary.
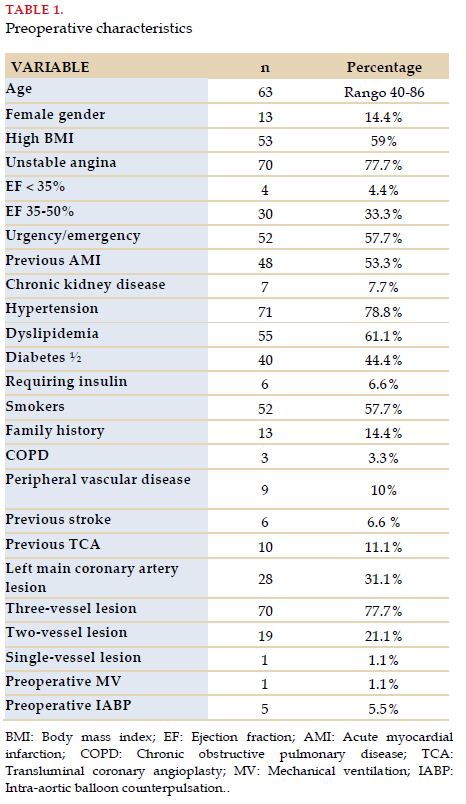
After previous administration of an appropriate dose of heparin, both previously skeletonized internal mammary arteries are dissected. In the case of performing two or three bypasses, the free right internal mammary artery (RIMA) is anastomosed to the left internal mammary artery (LIMA) in situ in T, at the root of the pulmonary artery, using the stabilizer and a glove retractor to come up with a “tiny plateau” to facilitate suturing.
When it was necessary to use the saphenous vein, proximal anastomosis was performed on the aorta, with partial clamping, whether before or after distal anastomosis, according to the case. It was used in patients requiring 4 bypasses, or when the risk of sternum infection was high.
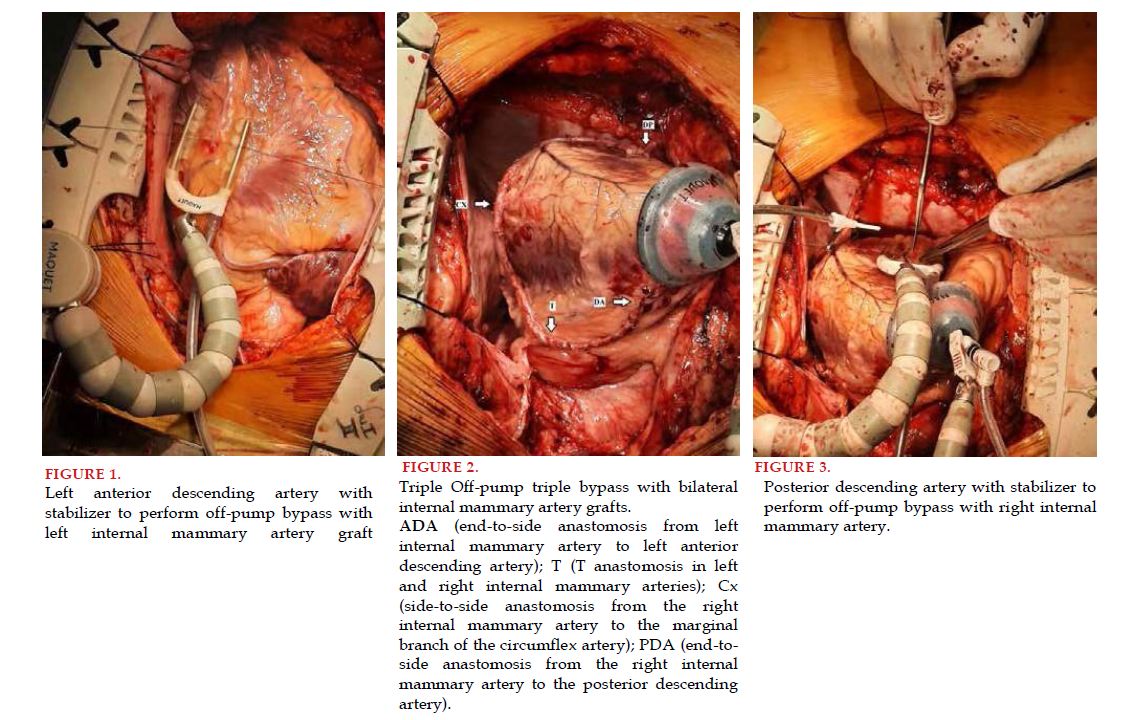
First, the anterior descending artery (ADA) is revascularized applying a routine shunt to maintain coronary circulation by proximal compression control during placement (Figure 1).
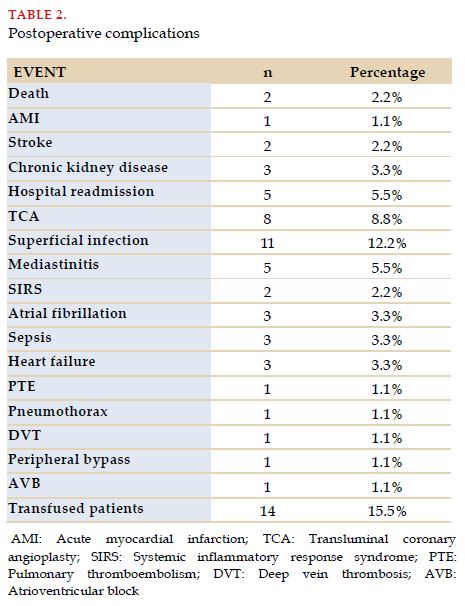
After ADA revascularization, the tip suction device is placed, it is verified whether the RIMA reached the right coronary artery (RCA) when necessary and the location where the circumflex artery (Cx) side-to-side anastomosis will be performed with 6-0 silk sutures, which will help as support during arteriotomy. The same process is carried out in the case of revascularizing a diagonal or lateral branch of the circumflex artery (Figure 2). The last anastomosis, whether in the marginal branch of the LCx or the posterior descending artery (PDA), is made in an end-to-side way (Figure 3).
Polypropylene sutures are used, with sizes 8-0 for arterial anastomoses, 7-0 for distal venous anastomoses and 6-0 for the proximal anastomoses.
The gurney is put in a lateral position toward the surgeon for the Cx anastomosis and Trendelenburg position is used for the RCA.
After controlling hemostasis, anticoagulation is reversed with protamine and controlled by activated clotting time (ACT).
Closure is made by the usual technique, leaving a temporary pacemaker (TPM) and mediastinal and pleural drains if the pleurae open. Extubation is attempted in patients in the OR.
RESULTS
The pre-operative characteristics of patients are described in Table 1.
Most were men, with an average age of 63 years, with high BMI, who had been admitted due to unstable angina. A high percentage were operated during admission, whether due to the severity of the lesion, instability of patients, or because moving them was inconvenient, since most were referred from distant centers within the Patagonian region.
The first one experienced an acute myocardial infarction (AMI) and cardiorespiratory arrest (CRA) when already in the general ward, with suspicion of occlusion in venous bypass to RCA. Although there were no re-interventions by bleeding, this patient suffered a considerable pharmacological bleeding that was corrected. He was reanimated and studied again, with the venous bypass opening, but he had no neurological sequelae and died one month after the intervention. .
The second patient was a surgical rescue, in a patient with AMI, mechanical ventilation (MV), in dialysis, with intra-aortic balloon counterpulsation (IABP). ADA and PDA were revascularized, and coronary angioplasty was conducted from the marginal branch to the Cx the following day. He evolved better than expected, but during the third week after the surgery, he experienced a CRA with reanimation, dying days later. .
There were no strokes related to the procedure proper. One patient suffered severe hypotension after AMI dissection that required cardiac massage, reverting it and stabilizing him with pharmacological support. The procedure continued, presenting mild postoperative sequelae that reverted immediately.
Perioperative AMI was diagnosed in one patient. Postoperative TCA was conducted in 8 patients, mostly in territories with previous AMI and poor sites. Three required TCA within the hospitalization period: one patient due to intramuscular Cx difficult to reach and another due to suspicion of lesion in LIMA-to-ADA anastomosis, where the RCA was also dilated and with underestimated moderate lesion
Fourteen patients received transfusions with deplasmatized erythrocytes. Two of them also required platelets, and one, cryoprecipitates. Most transfused patients presented complications, prolonged hospital stays, or were in dialysis.
Eleven patients had superficial infections that were solved with antibiotic treatment and wound cleaning and dressing. Five developed mediastinitis, of whom 4 required a revision. In one of them, a single mammary artery was used. The other 3 were in dialysis, with multiple risk factors. Bilateral internal mammary artery grafts were made in two of them as they were younger than 50 years, and a third by previous bilateral saphenectomy. The VAC system was used when the revision was not effective to close the wound. One patient had a poor course, with sepsis, and finally died .
Another patient died after 2 months due to heart failure and sepsis, with history of drug addiction. Mortality in the long term was then 4.4% (4 patients).
The average of hospital-stay days since admission was 11.5; and after the surgery, it was 7.1. More than 50% of patients were discharged before the 5th day after undergoing surgery.
DISCUSSION
In spite of heart surgery having started with a beating heart, with the advent of cardiopulmonary bypass and cardioplegia, interest was lost on a more demanding technique. By mid-1990s, interest was strengthened again, helped by technical advancements on stabilizers[1,2].
From reading Table 1, it emerges that the cohort of patients studied constitutes a high risk group for any surgery, on or off-pump, but this was not an obstacle to indicate it. In other words, there was no selection of patients looking for an improvement in the final outcome of the procedure. As there were no patients with on-pump surgeries to establish comparisons in terms of differences in mortality with off-pump patients, it is improper to draw conclusions about it; although we have the intuition that on-pump would have probably increased morbimortality to a degree. In this regard, the comparative studies show varied results. One of the most important ones, the CORONARY trial with 4752 patients from 79 centers in 19 countries, intervened with both techniques, concluded that there were no significant differences in terms of primary aims in one year, as long as off-pump MRS was performed by surgeons experienced in this technique[3].
Bypass permeability is one of the most influential factors on coronary artery surgery outcome, which is measured by the percentage of re-interventions and mortality[4]. It is well known that off-pump surgery entails a learning curve that has been estimated in around 50 cases. This may explain anastomoses failures or the need for post-operative TCA in some cases. A proper strategy and proper choice of grafts allow ensuring complete revascularization, and high anastomoses permeability in off-pump surgery.
Using bilateral internal mammary artery grafts, avoiding touching the aorta, prevents the complications that may arise from it[5]. When performed in T, it provides a proper circulation, thus enabling revascularization in all sectors of the heat, with the subsequent benefits over time in regard to the need of distant revascularization. When skeletonized, the risk of mediastinitis is reduced, even in diabetic patients[6].
Avoiding cardiopulmonary bypass prevents a systemic inflammatory response, decreases multiorgan damage, favors early extubation and decreases post-operative bleeding rates. Those who benefit the most are patients older than 75 years[1,7,8].
We should mention the financial considerations of this surgery, mainly by decreasing the time of hospital stay[9].
Using IABP contributes to the reduction of postload, but does not influence coronary circulation because of coronary self-regulation, which could be affected during on-pump surgery[7]. It is used as support in selected patients with poor ventricular function and/or very severe LMCA lesions.
As limitations of the study, we should highlight the size of the sample and their control over time
CONCLUSIONS
Off-pump coronary surgery with bilateral internal mammary artery grafts is a safe procedure, with low morbimortality. Surgeon’s experience is important when performing the procedure, with the possibility of most patients being revascularized, not requiring on-pump surgery, even with low EF and difficult anastomosis. A rigorous shunt use, delicately positioning the heart and being helped by the positions of the gurney are some of the strategies to revascularize all regions of the heart. Having the heart beating allows to realize whether it is under stress to reposition it or to change the strategy. Inotropic drugs and IABP may help in specific situations. The help of anesthetists is extremely important in all stages of the procedure. The benefits of revascularization become evident almost immediately in most cases. There is no doubt that patients benefit from a faster recovery, not limiting the outcome.
The authors would like to thank Dr. Alberto José Canestri for his collaboration in reviewing the manuscript.
BIBLIOGRAPHY