1 Instituto de Cardiología y Cirugía Cardiovascular. Posadas, Argentina. 2 Universidad Católica de las Misiones. Posadas, Argentina. 3 Hospital Universi- tario Ramón y Cajal. Madrid. España. 4 Sanatorio Finochietto. Sanatorio FLENI. Ciudad Autónoma de Buenos Aires.
Corresponding author’s address
Dr. Gerardo Moreno
Unidad de Arritmias. Instituto de Cardiología y Cirugía Cardiovascular
Santiago del Estero 2369
3300. Posadas. Misiones
Cellphone: 3764355375
Fax: 3764431855 Ext: 154
E-mail
Received on March 1, 2022 Accepted after review on April 14, 2022 www.revistafac.org.ar
There are no conflicts of interest to disclose.
Keywords:
Hypertrophic cardiomyopathy.
Atrial Arrhythmias.
Electrocardiogram. Atrial Fibrillation
ABSTRACT
Introduction: Electrocardiographic tracing plays an important role in the diagnosis and prog- nostic stratification of patients with Hypertrophic Cardiomyopathy (HCM) .
Objectives: To determine the electrocardiographic signs present in these patients and their correlation with the prevalence of isolated atrial arrhythmias and self-limited bursts that could create a predictive pattern of Atrial Fibrillation.
Material and methods: Observational, descriptive, cross-sectional, and statistical correlation study of Spanish and Argentine patients with HCM in whom anamnesis, physical examination, electrocardiogram, transthoracic Doppler echocardiogram and Holter study were performed.
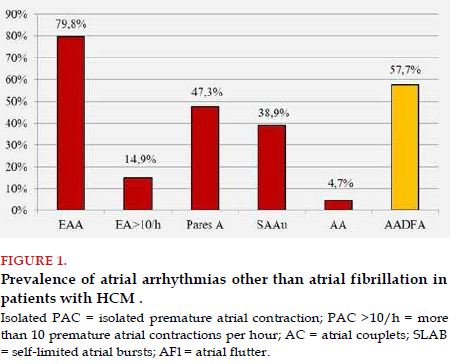
Results: There were 117 patients included, mean age 47 years, 56% male. The prevalence of isolated premature atrial contractions (PACs) was 79.8%, high density of PACs 14.9%, atrial couplets 47.3%, self-limited atrial salvoes 38.9%, atrial flutter 4.7%, and atrial arrhythmias other than atrial fibrillation (AAOAF) 57.7%. The electrocardiographic signs that were statistically correlated with the presence of AAOAF were P wave ≥100 ms, P wave dispersion <40 ms, QRS duration >80 ms, the presence of high density of isolated premature ventricular contractions (PVCs) and non-sustained ventricular tachycardia salvoes in Holter study. The presence of pathological Q waves showed just a statistical trend.
Conclusions: In patients with HCM, AAOAF showed a high prevalence and were associated with an electrocardiographic pattern composed of P wave ≥100 ms, P dispersion <40 ms, QRS >80 ms, PVCs >10/hour, NSVT. This pattern could be associated with the development of AF in patients with HCM.
INTRODUCTION
In patients with hypertrophic cardiomyopathy (HCM), atrial arrhythmias are frequent; among them: atrial fibrillation (AF), which appears in 22.5% of cases, and entails a high risk of both central and peripheral ischemic vascular complications, alters the patient’s quality of life, is closely associated to heart failure, to cognitive impairment, and doubles mortality in patients suffering from it[1,2]. Everything that clinical research may contribute to prevent, diagnose and avoid the inherent complications of AF in patients with HCM is always welcome and very useful.
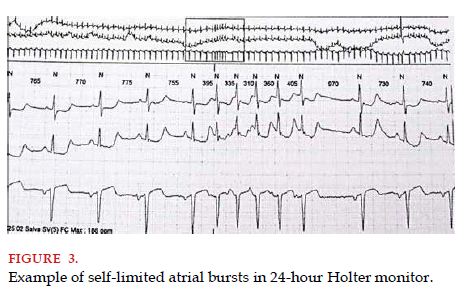
There is little information of atrial arrhythmias other than AF (AAOAF) in these patients, such as isolated premature atrial contractions (PACs), atrial couplets (AC), self-limited atrial bursts (SLAB) and atrial flutter (AFl), which often are known AF predictors[3,4,5,6].
.
The electrocardiographic tracing (ECG) plays a leading role in the diagnosis, prognosis and therapeutic management of patients with HCM. Its usefulness has not lost relevance, in spite of the remarkable advancement of technology applied to auxiliary methods in medicine.
For this reason, it was considered convenient to describe and correlate the electrocardiographic signs shown in patients with HCM and their association with the prevalence of AAOAF, and thus determine the prevalent electrocardiographic pattern, which could be used as a new predictor tool for AF in this population.
MATERIALS AND METHODS
An observational, retrospective, descriptive, cross-sectional and statistical correlation study was conducted, where Spanish and Argentine patients were included, with diagnosis of HCM according to the definition proposed by the 2014 ESC Guidelines, who were evaluated at the Unit of Arrhythmias of the Hospital Universitario Ramón y Cajal of the city of Madrid, Spain, from year 2004 to 2007; and at the Unit of Arrhythmias of the Instituto de Cardiología y Cirugía Cardiovascular of the city of Posadas, Misiones, Argentina, from year 2014 to 2018[1]. Patients were excluded when: they had diagnosis of paroxysmal, persistent or permanent atrial fibrillation, and when they didn’t give their consent to perform the indicated auxiliary tests and/or to use their data for the clinical investigation. The international criteria of confidentiality were met at all times.
The medical evaluation consisted of anamnesis and physical examination, performance of standard 12-lead ECG, transthoracic Doppler echocardiogram and Holter monitor test.
AAOAF were defined as isolated premature atrial contractions, couplets, self-limited bursts and atrial flutter. High density of PACs was defined as a number equal or above 10 isolated PACs per hour and/or the presence of SLABs. The latter was defined as three or more consecutive PACs, with an atrial rate of 120 bpm or more, and spontaneous cessation before 30 seconds.
A database was created with the SPSS19 software and statistical tests were conducted
.
RESULTS
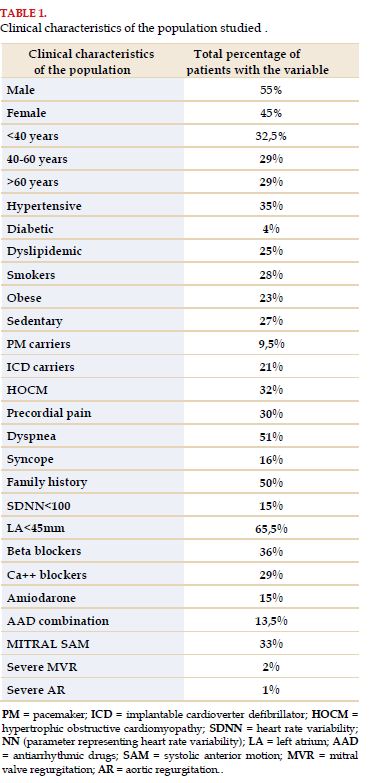
The population included in the study was constituted by 117 patients with diagnosis of hypertrophic cardiomyopathy, with average age of 47 years (range between 13 and 84 years), and 56% were males. The prevalence of cardiovascular risk factors in the population studied and their clinical profile were previously published[7].
The clinical characteristics of the population studied are shown in
Table 1 .
The presence of atrial arrhythmias in the Holter monitor test of patients included was high: 79.9% presented isolated PACs, with high density of presentation in 15% of cases; 47% presented atrial couplets and 39% self-limited atrial tachycardia runs (Figure 1).
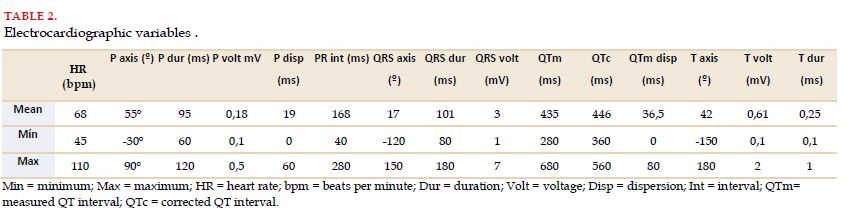
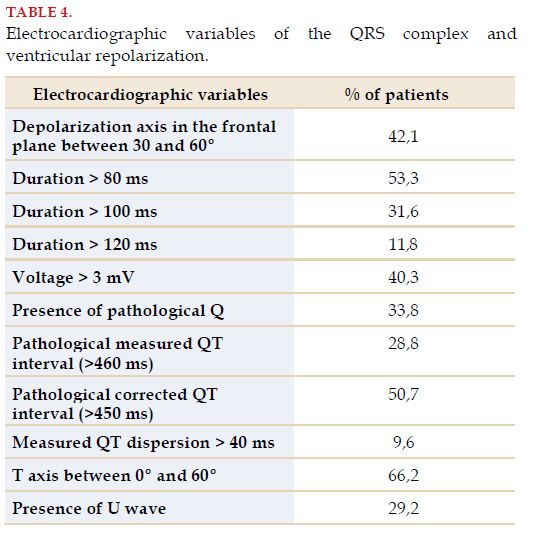
The percentage of patients that presented 1st degree AV block (PR interval ≥200 ms) was 5.6%. No major AV conduction disorders were recorded in the patients studied. The characteristics recorded of the QRS complex and ventricular repolarization are shown in (Table 4) .
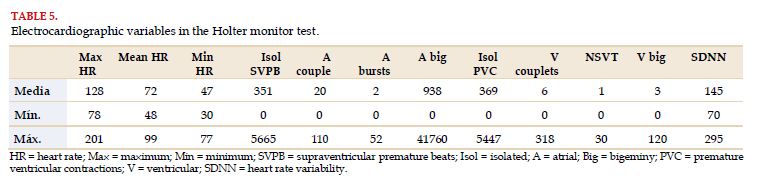
In 33% of cases there were episodes of bradycardia, and 3% had sinus pauses of more than 2 seconds recorded (all of them between 2 and 2.8 seconds of duration).
Heart rate variability expressed in the standard deviation of NN (SDNN) was pathological (<100 milliseconds) in 18% of patients.
When correlating the electrocardiographic signs of patients, included with the presence of AAOAF, we may observe the results shown in Table 6.
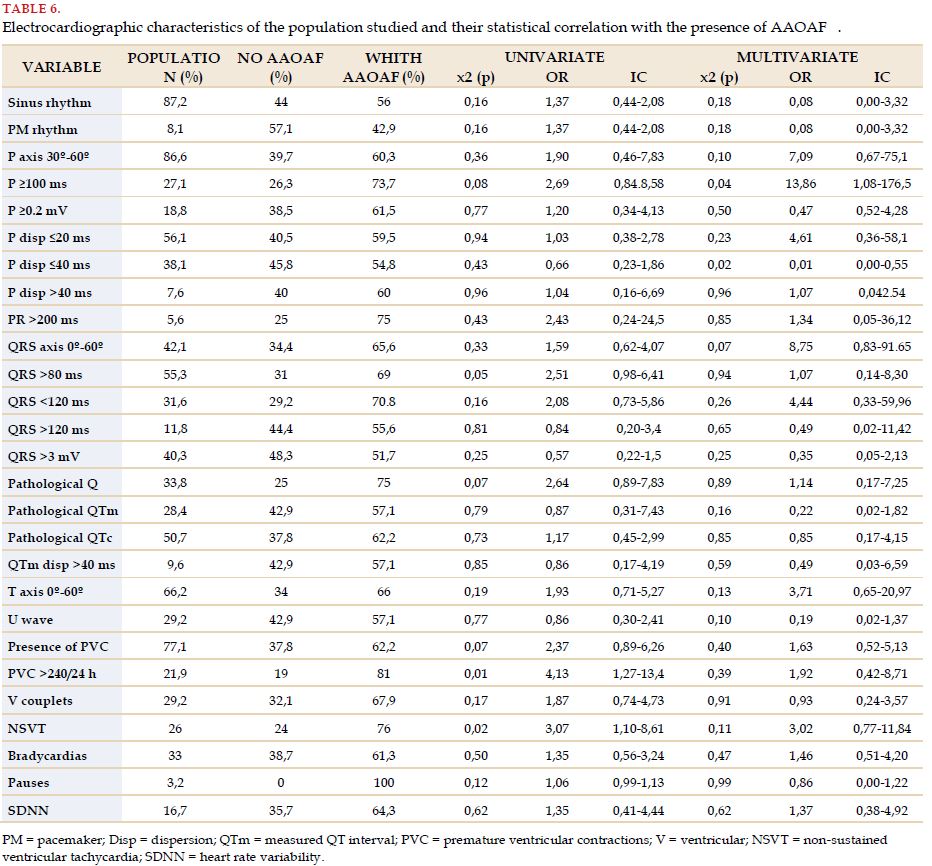
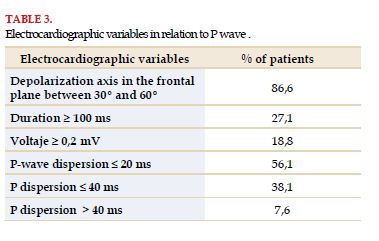
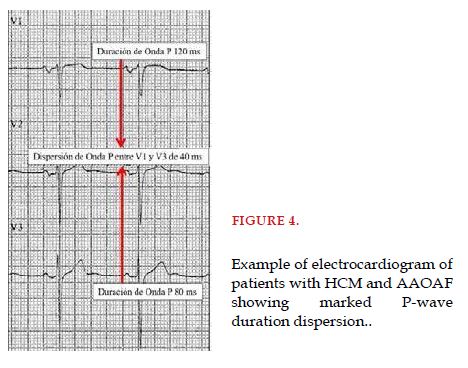
P wave duration ≥100 ms showed a statistical association in the multivariate analysis with the presence of AAOAF. Likewise, P wave duration dispersion ≤40 ms was statistically associated with the presence of AAOAF in multivariate analysis.
QRS complex axis between 0º and 60º (normal), as well as the presence of pathological Q wave, showed only a statistical trend with the presence of AAOAF. An electrocardiographic parameter that represents ventricular activation time reached a statistical association. QRS complex width >80 ms is associated to a greater prevalence of AAOAF in patients with HCM in univariate analysis.
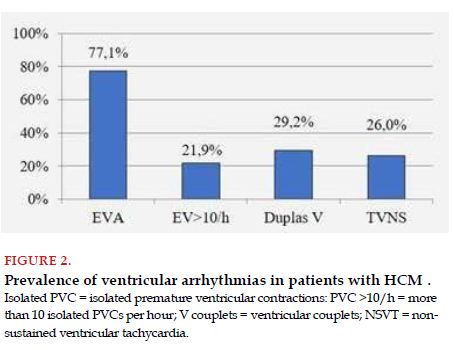
Between the electrocardiographic variables obtained in the Holter monitor test, the presence of isolated PVCs displayed only a statistical correlation trend; but the high density of PVCs (more than 10 per hour) and the presence of NSVT showed a clear association in univariate analysis with the presence of AAOAF.
Finally, and taking into account the descriptive statistics as a whole and the contingency table performed to assess the statistical correlation (uni and multivariate analysis), certain characteristics become evident, which would constitute a prevalent electrocardiographic pattern in patients with HCM and AAOAF
DISCUSSION
In this study, there is a significant density of atrial arrhythmias present in patients with HCM: 57.7% of them presented AAOAF.
Identifying an electrocardiographic pattern, statistically associated to the presence of AAOAF, which represent an important trigger for AF, becomes very relevant in patients with HCM, because of the high incidence and severe consequences that AF causes.
This study achieves its goal, showing statistical associations that help to constitute a prevalent electrocardiographic pattern in patients with HCM and AAOAF.
The electrocardiogram, the initial auxiliary test in any patient with HCM, very useful both for diagnostic screening and the follow-up and prognosis of the patient, is characterized by presenting some anomaly in 75% to 95% of cases[8].
Regrettably, many patients with HCM present stroke as the first clinical manifestation of AF[9]. The capacity of a noninvasive study, such as the electrocardiogram, to identify patients in high risk of stroke related to AF and to start prophylactic anticoagulation is invaluable.
Noninvasive markers of AF, such as electrocardiographic parameters, also help to evaluate the response to pharmacological antiarrhythmic and/or interventionist therapy (ablation), and to identify patients that may probably have atrial disease progressing. For all of these reasons, thoroughly studying electrocardiographic parameters and creating a risk profile becomes relevant.
In this investigation study, once again there was a statistical association between P-wave duration with the prevalence of atrial arrhythmias, just as it had already been verified by other investigators[10,11]. P-wave duration ≥100 ms showed a correlation in multivariate analysis with the presence of AAOAF, and in turn, the dispersion of its duration in surface ECG, when said dispersion did not exceed 40 ms, was also associated to AAOAF.
Both electrocardiographic parameters, very simple for evaluation, contribute much information to be one step ahead of the possible development of AAOAF, and probably, be ahead of AF development.
It was possible to observe also, that when QRS is >80 ms, it correlated statistically with the presence of AAOAF, which leads us to think that the greater the electrical compromise at the level of ventricular depolarization, probably due to greater ventricular myocardial tissue disruption, the more atrial myocardial tissue disruption there would be too, and hence, the greater the prevalence of AAOAF.
LIMITATIONS
This is a retrospective study of patients who were referred to tertiary health care centers for evaluation and treatment; therefore, it may not reflect the reality of all patients with HCM. Also, we should consider the sporadic presentation and variability over time of the studied arrhythmias, which conditions the sensitivity of the Holter monitor test for their detection
CONCLUSIONS
AAOAF are frequent in patients with HCM. A P wave ≥100 ms, P wave dispersion ≤40 ms, QRS >80 ms, presence of pathological Q wave in ECG, and of high density of isolated ventricular arrhythmias and NSVT runs in Holter monitor correlate to the presence of AAOAF. Because AAOAF are important AF triggers, the electrocardiographic pattern described may identify patients with HCM and high chances of developing AF.
SPECIAL ACKNOWLEDGEMENTS
To Prof. Dr. Concepción Moro Serrano and Prof. Dr. Antonio Hernández Madrid, of the Hospital Ramón y Cajal, of the city of Madrid, Spain; my teachers of cardiac electrophysiology and pacing, because of their invaluable guidance and permanent encouragement for the investigation of hypertrophic cardiomyopathy.
BIBLIOGRAPHY